The NIH Stroke Scale
Medical professionals and even the public have been trained to recognize basic signs of stroke. These include three features of stroke: slurred speech, drooping of one outstretched arm, and drooping of one side of the face when attempting to smile. When one of these signs is present it’s a fairly sensitive indicator of stroke. When all three are present, sensitivity for stroke is approximately 90%. However, when evaluating patients for inclusion in stroke protocols and prior to fibrinolytic stroke treatments, medical professionals use a slightly more sophisticated series of questions. They often use the NIH stroke scale.
The NIH offers training and certification in the administration and scoring of the stroke scale. An overview of the scale is listed below.
The stroke scale items should be presented in order and the score should be reported after each numbered category has been assessed. The score should be based on the patient’s actual performance and what is witnessed by the examiner. It should not be a reflection of what the examiner thinks the patient is able to do. Remember, the patient could be experiencing an acute stroke, so time is of the essence. The examiner should work quickly. On the other hand, the patient should not be coached or aided by anyone, including the examiner. If the patient cannot perform one of the items, indicate the corresponding score, and move onto the next item.
National Institutes of Health (NIH) Stroke Scale
| 1a. Level of consciousness | 0 = Alert and responsive
1 = Arousable to minor stimulation 2 = Arousable only to painful stimulation 3 = Unarousable or reflex responses |
| 1b. Questions
Ask patient’s age and month. Must be exact. |
0 = Both correct
1 = One correct 2 = Neither correct |
| 1c. Commands
Ask patient to open/close eyes, grip and release non-affected hand. |
0 = Both correct
1 = One correct 2 = Neither correct |
| 2. Best gaze
Horizontal extraocular movements by voluntary or reflexive testing. |
0 = Normal
1 = Partial gaze palsy; abnormal gaze in one or both eyes 2 = Forced eye deviation or total paresis which cannot be overcome by oculocephalic maneuver |
| 3. Visual fields
Test by confrontation or threat as appropriate. If monocular, score field of good eye. |
0 = No visual loss
1 = Partial hemianopia, quadrantanopia, extinction 2 = Complete hemianopia 3 = Bilateral hemianopia or blindness |
| 4. Facial palsy
If stuporous, check symmetry of grimace to pain. Paralysis (lower face). |
0 = Normal
1 = Minor paralysis (normal looking face, asymmetric smile) 2 = Partial paralysis 3 = Complete paralysis (upper and lower face) |
| 5a. Left motor arm
5b. Right motor arm
Arms outstretched 90° (if patient is sitting) or 45° (if supine) for 10 seconds. Encourage best effort, note paretic side. |
0 = No drift
1 = Drift but does not hit bed 2 = Some antigravity effort, but cannot sustain 4 = No movement at all X = Unable to assess due to amputation, fusion, etc |
| 6a. Left motor leg
6b. Right motor leg
Raise leg to 30° (always test patient supine) for 5 seconds. |
|
| 7. Limb ataxia
Check finger-nose-finger; heel-shin; score only if out of proportion to weakness. |
0 = No ataxia (or aphasic, hemiplegic)
1 = Ataxia present in one limb 2 = Ataxia present in two limbs X = Unable to assess as above |
| 8. Sensory
Use safety pin. Check grimace or withdrawal if stuporous. Score only stroke related losses. |
0 = Normal
1 = Mild to moderate unilateral sensory loss but patient aware of touch 2 = Severe to total sensory loss, patient unaware of touch (or bilateral sensory loss or comatose) |
| 9. Best language
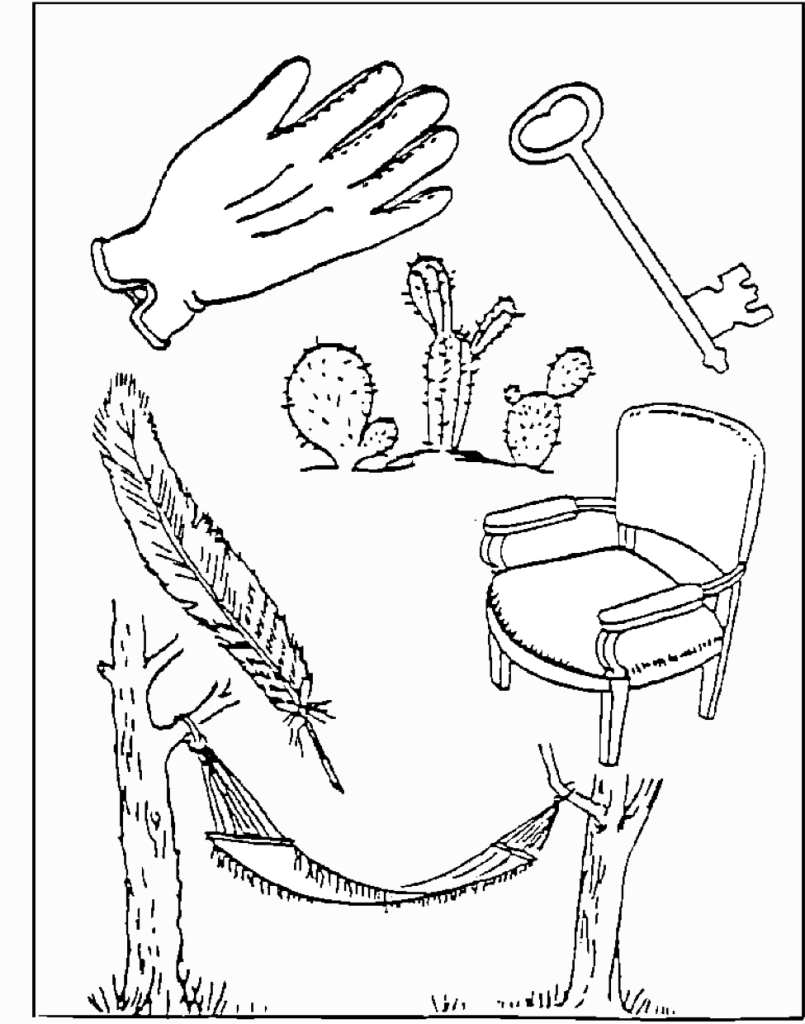
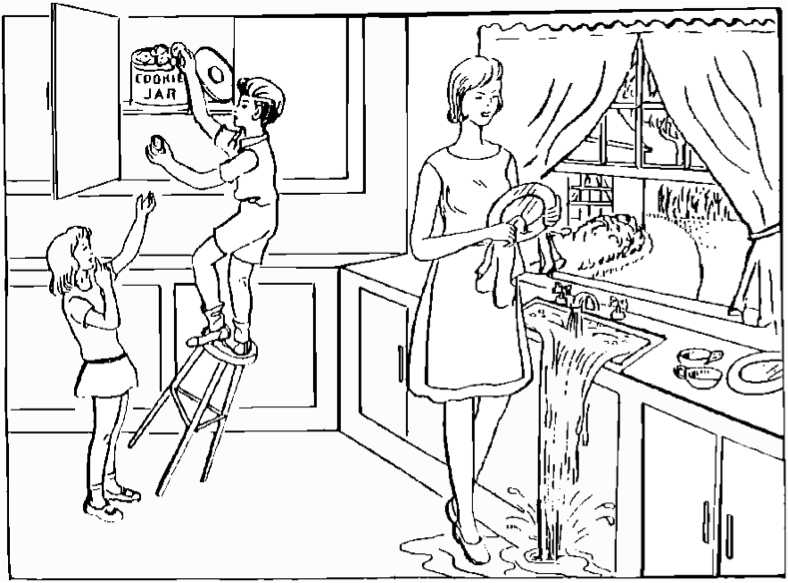
Ask patient to describe cookie jar picture, name objects, read sentences. May use repeating, writing, stereognosis. |
0 = Normal
1 = Mild-moderate aphasia 2 = Severe aphasia (almost no information exchanged) |
| 10. Dysarthria
Ask patient to read or repeat a list of words. |
0 = Normal
1 = Mild-moderate dysarthria 2 = Severe, unintelligible or mute X = Intubation or mechanical barrier |
| 11. Extinction and inattention
Simultaneously touch patient on both hands, show fingers in both visual fields, ask patient to describe deficit, left hand. |
0 = Normal, none detected (or severe visual loss with normal cutaneous responses)
1 = Neglects or extinguishes to bilateral simultaneous stimulation in any sensory modality (visual, tactile, auditory, spatial, or personal inattention) 2 = Profound hemi-inattention or extinction in more than one modality |
Most people receive a score 0 after taking the NIH stroke scale. Scores as low as one to four could indicate a mild stroke. The highest possible score is 42 which would obviously be consistent with a profound stroke. The NIH stroke scale can be administered in less than 10 minutes in skilled hands. It provides excellent baseline for stroke treatment assessment and can be used for prognosis.
Images used with the NIH Stroke Scale:
You know how.
Down to earth.
I got home from work.
Near the table in the dining room.
They heard him speak on the radio last night.