
Treating Supraventricular Tachycardia with Adenosine
EMS is called to a local medical clinic for a 53 year old female complaining of weakness and palpitations.
Symptoms started earlier in the day at tennis camp. The patient experienced one other episode about 2 years prior that proved to be self-limiting.
She takes no medications and has no known drug allergies.
The patient appears anxious but is oriented to person, place, time, and event.
Vital signs are assessed:
- HR: 200
- NIBP: 134/102
- RR: 18
- Temp: 98.4 F
- SpO2: 95% on RA
- BGL: 88
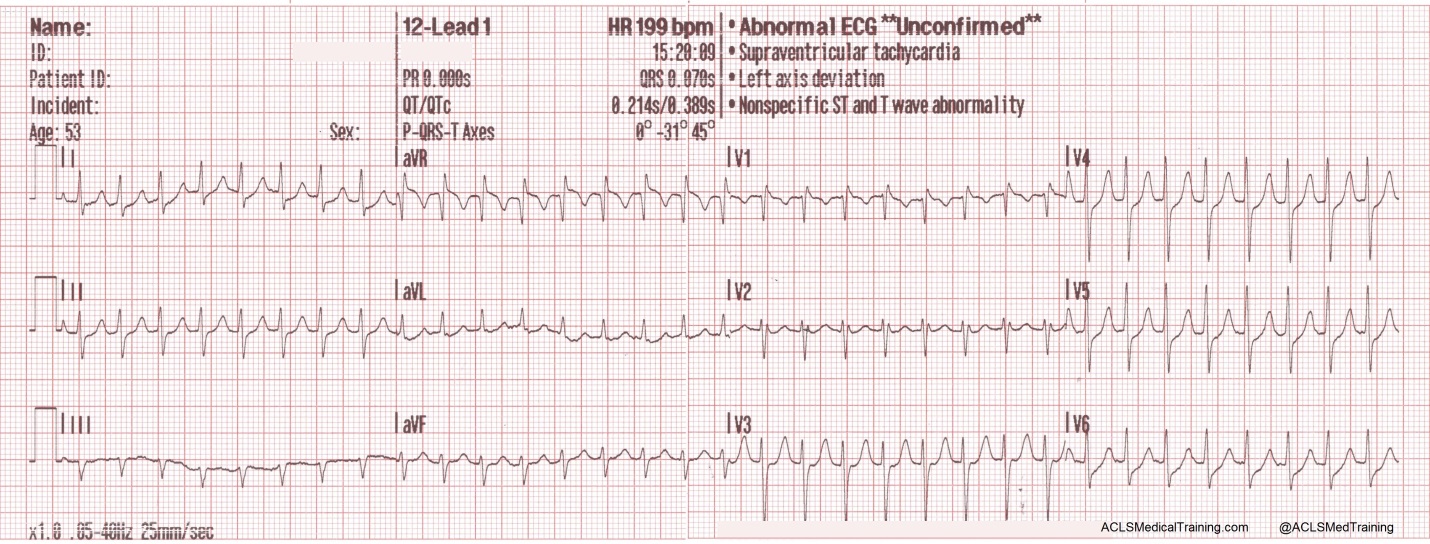
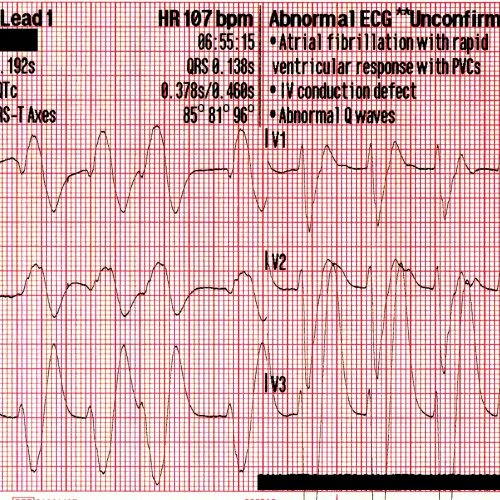
A 12-lead ECG is obtained by paramedics.
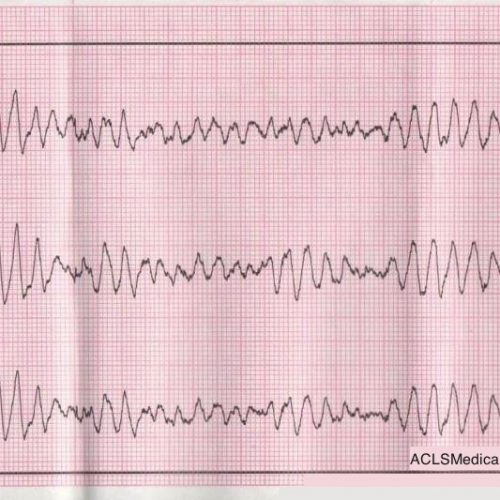
A rhythm strip is also recorded.
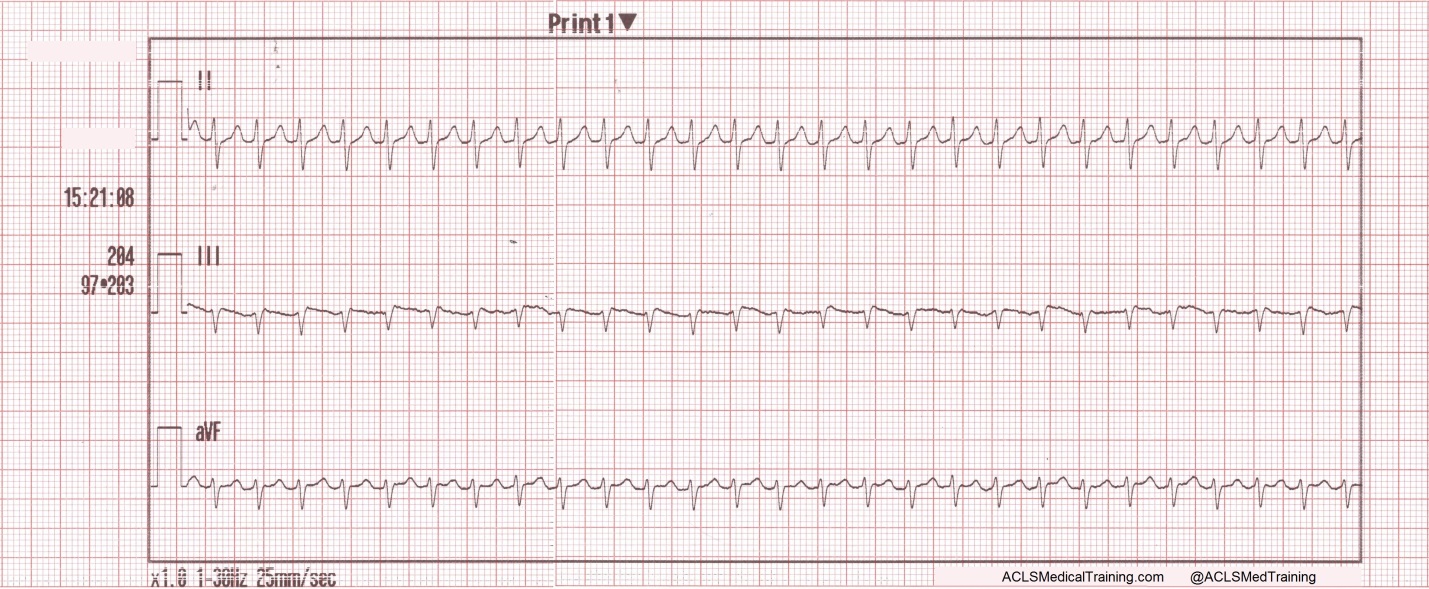
Paramedics note a regular narrow complex tachycardia at a rate of about 200/min.
Could this be sinus tachycardia?
It is doubtful. There are no visible P-waves. In addition, the maximum theoretical sinus rate is 220 minus age (plus or minus 10%). For this patient that works out to somewhere between 167 and 184.
Vagal maneuvers are attempted but are unsuccessful.
As a side note, the REVERT Trial which was published this year introduced a postural modification (leg elevation and supine positioning) to the standard Valsalva maneuver for the treatment of SVT which returned 40% of patients to sinus rhythm compared with 17% for the standard Valsalva maneuver.
You can watch a video of the technique here: https://www.youtube.com/watch?v=8DIRiOA_OsA
In this case, an IV is started and 12 mg of adenosine is given rapid IV push followed by a 20 ml syringe bolus of 0.9% normal saline.
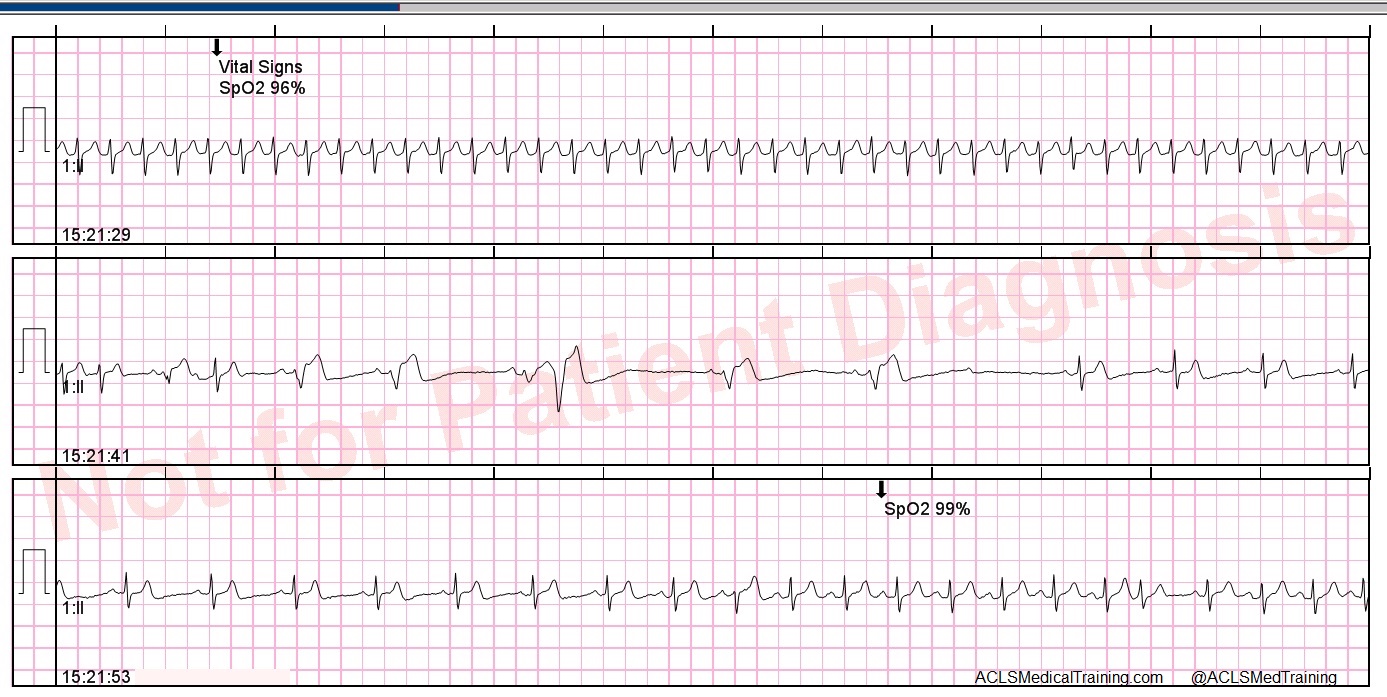
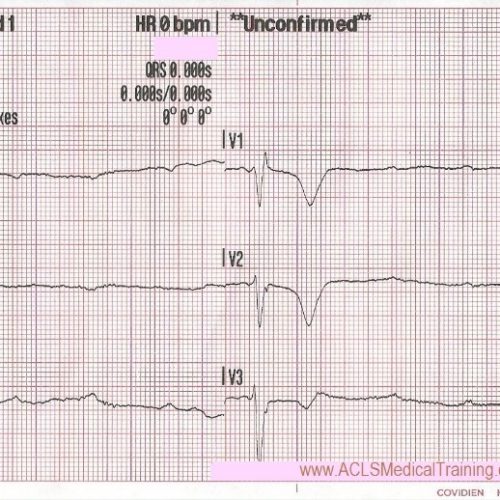
The rhythm is successfully converted and another 12-lead ECG is obtained.
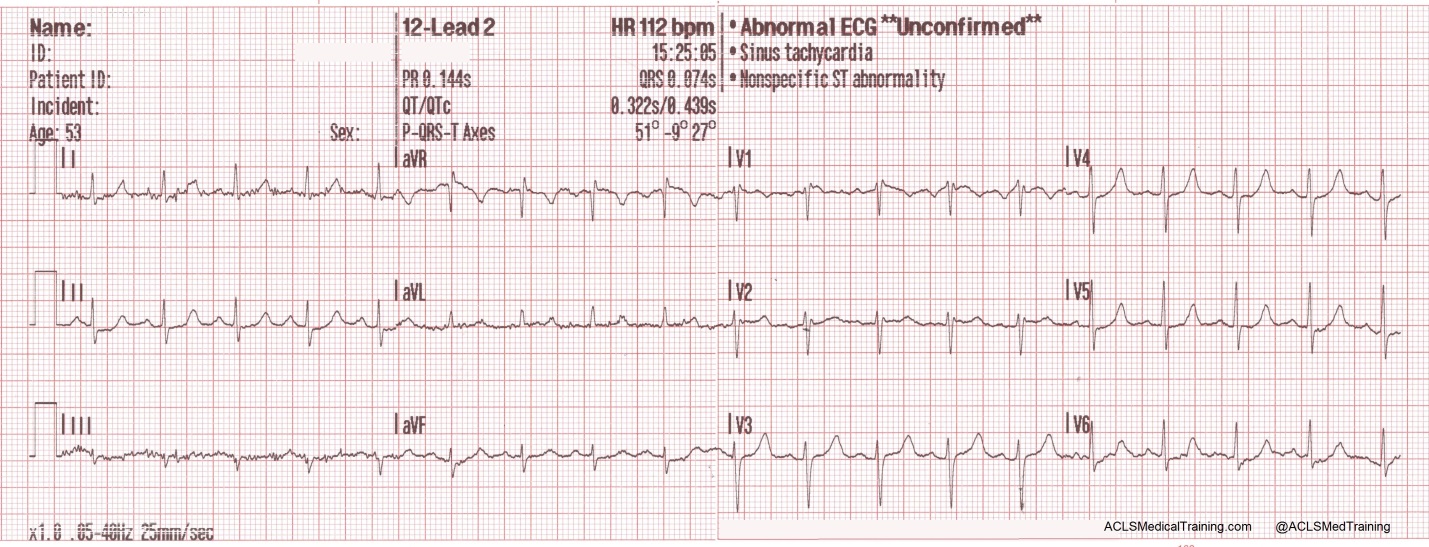
It should be noted that modest nonspecific ST/T wave abnormalities are not uncommon immediately following the conversion of SVT to sinus rhythm. The main determinant of myocardial oxygen demand is heart rate!
Take-away points
The maximum theoretical sinus rate is 220 minus age (plus or minus 10%).
Adenosine should be used for regular tachycardias only! It can be dangerous in the setting of atrial fibrillation and Wolff-Parkinson-White Syndrome.
Record a 12-lead ECG whenever possible prior to treating a narrow complex tachycardia with adenosine. It can be helpful later on when the patient is referred to a cardiologist or electrophysiologist.
Consider a postural modification (leg elevation and supine positioning) to the Valsalva maneuver to improve the conversion rate.
Consider applying defibrillation pads prior to the administration of adenosine.
The drugs Dipyridamole (Persantine) and Carbamazepine (Tegretol) can potentiate adenosine.

Comments