
Posterior STEMI and Prehospital Tenecteplase (TNK)
EMS is called to the home of a 62-year-old female who complains of shortness of breath and epigastric discomfort.
On their arrival, they find the patient sitting on a chair in her living room, holding her hand to her chest while she talks with first responders. She is not pale, but appears diaphoretic, anxious, and has mildly laboured respirations.
A brief medical history is obtained while gathering a set of vitals and applying the ECG electrodes.
Onset: “It woke me up from my sleep”
Provocation: “Nothing makes it better or worse”
Quality: “Like heartburn, but worse”
Radiation: None
Severity: Rated 8 out of 10
Time: “About ninety minutes ago”
Pulse: 74/min, strong and regular at the wrist
RR: 20/min, clear air entry on auscultation
NIBP: 152/88
SpO2: 92% on room air
BGL: 7.4mmol/L (133 mg/dl)
Temp: 36.2C (97.2F)
PMHx : Hypertension, asthma, dyslipidemia
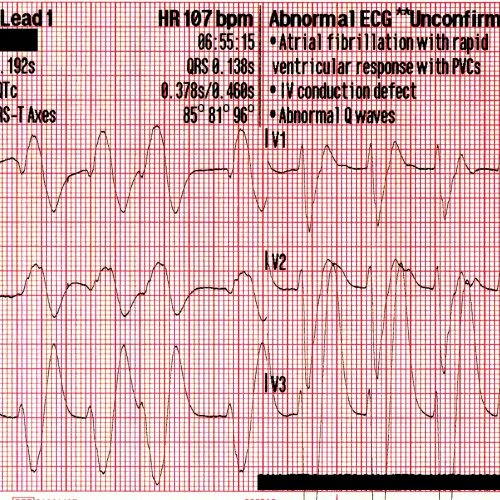
A 12-lead ECG is acquired.
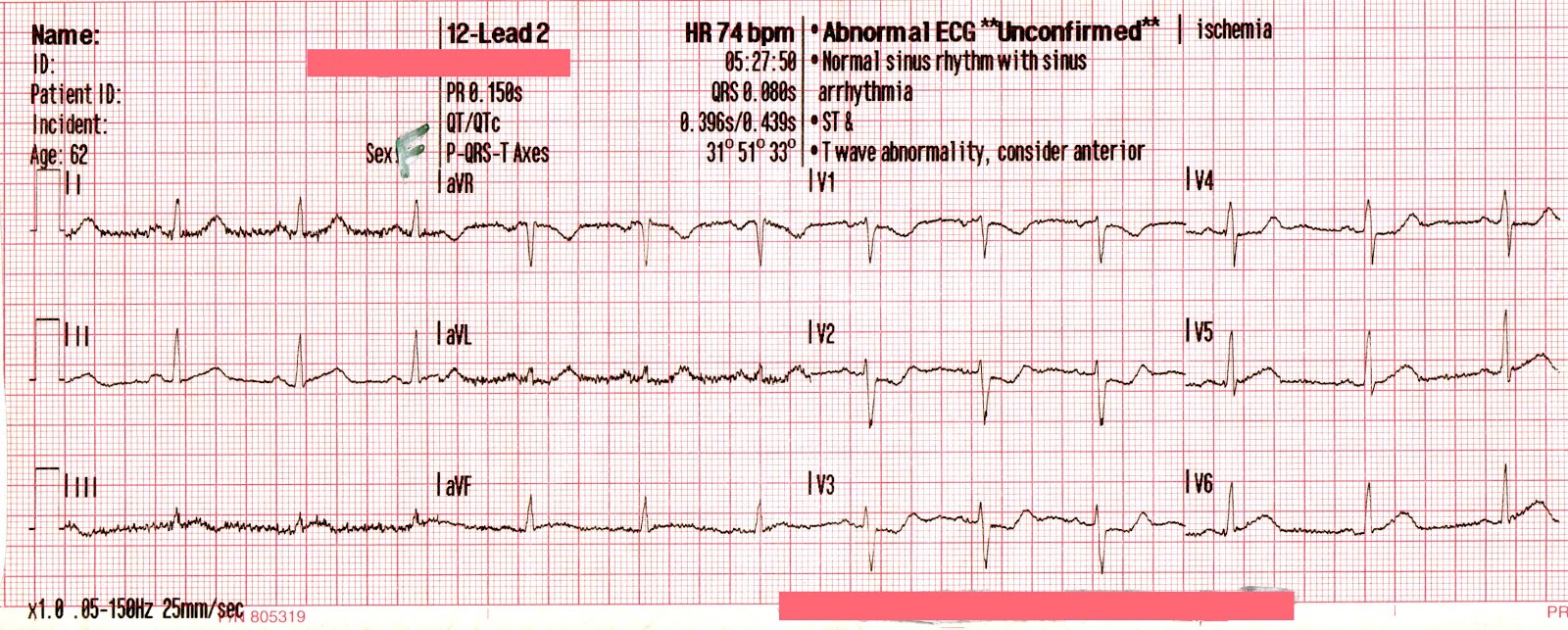
Sinus rhythm with some troubling ST depression in V2-V4. There is artifact in the limb leads, but nonetheless this ECG combined with the present physical findings is highly concerning for posterior STEMI.
At this point, the attending paramedic was highly suspicious that an acute coronary event was taking place, and proceeded to treat with Aspirin, SL Nitroglycerin, and serial 12-leads while initiating transport.
The following ECG was acquired with V4 moved to the position of V4R, and V5 & V6 moved to the position of V8 & V9, respectively.
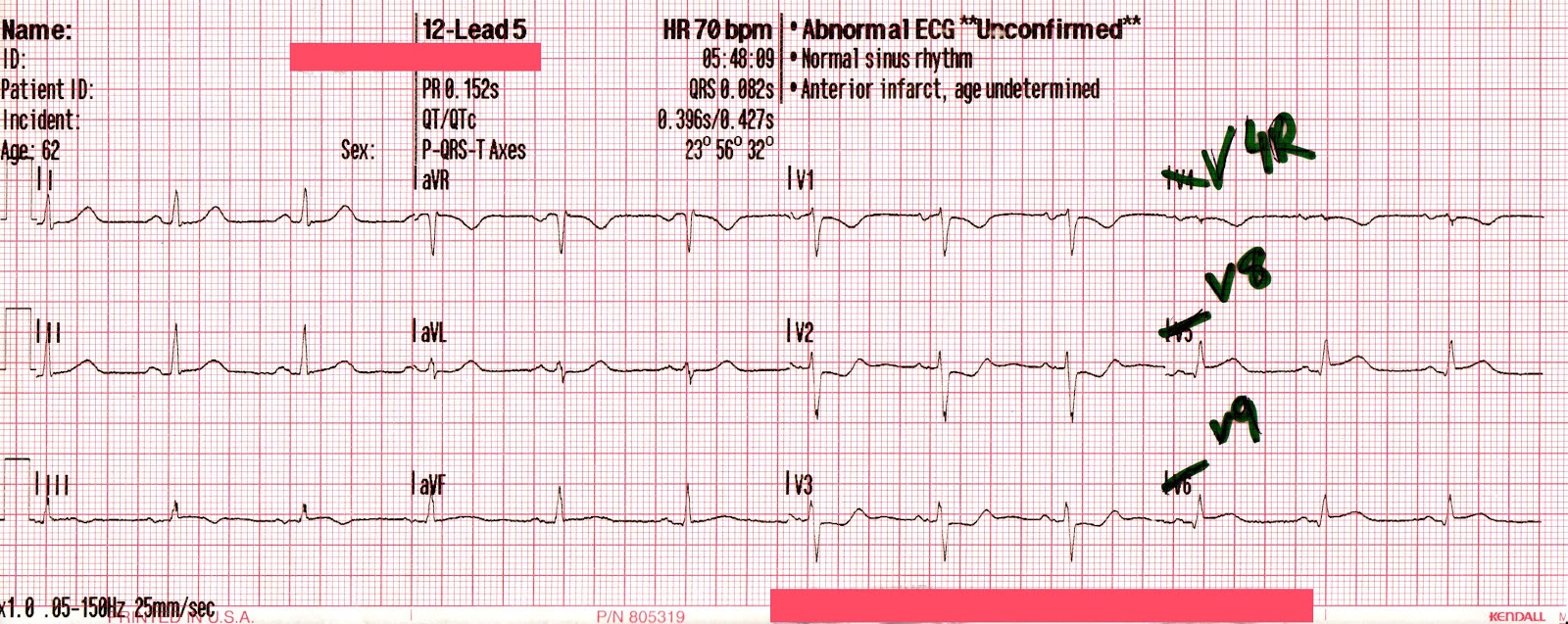
There is between 0.5 – 1.0mm of ST elevation in V8 and V9, and we can now appreciate T-wave inversions in lead III, perhaps indicating spontaneous occlusion/reperfusion of the RCA. This ECG is diagnostic of posterior STEMI.
The transporting paramedic recognized the posterior STEMI and transmitted the ECG to a consulting physician. Based on these findings, and considering the significant distance to a PCI-capable facility, the decision was made to administer Plavix and IV thrombolytics (TNK).
About 20 minutes post-TNK, it was noted that the patient’s heart rate had decreased to the low 40’s, while her chest discomfort simultaneously improved.
The following 12-lead was acquired.
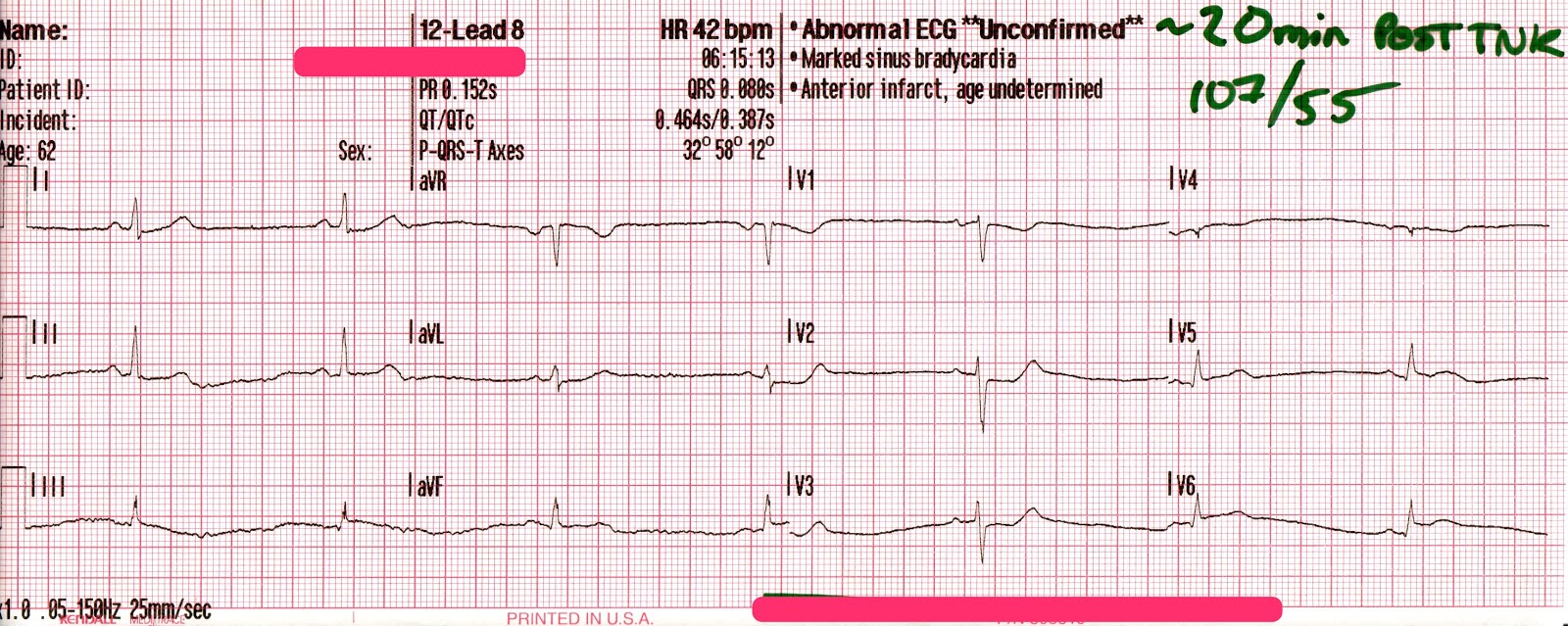
Sinus bradycardia. Note, leads V4, V5, and V6 still remain in positions V4R, V8, and V9 (respectively).
Despite the precipitous drop in blood pressure and heart rate, the patient appeared healthier now than she had at any point previously during the encounter.
Does this ECG represent improvement, or a decline in clinical condition?
Posterior STEMI
The diagnosis of a truly isolated posterior STEMI appears to be a relatively uncommon occurrence, presenting in about 3% of myocardial infarctions 1, however it’s highly likely that underdiagnosis has played a role in these underwhelming stats. This may be due to a misconception by many practitioners that ST Depression (STD) in leads V1-V3 represents anterior ischemia, despite the fact that myocardial ischemia does not localize on the 12-lead ECG.
This misinterpretation, combined with arbitrary millimeter criteria, often result in delayed cath lab activation, or a diagnosis of UA/NSTEMI in patients who are in fact suffering acute posterior STEMI.
There are several key criteria on the 12-lead ECG that, when observed in a patient suffering from a suspected acute coronary syndrome, should lead you to make the diagnosis of posterior STEMI. They include:
- Horizontal ST depression in V1-V3 with upright T-waves
- Early R-wave progression in the precordial leads
- ≥ 0.5mm ST Elevation (STE) in one or more posterior leads (V7-V9)*
* Due to the anatomical structures located between the posterior leads and the heart, there’s an increased amount of electrical impedance, which results in the appearance of much smaller QRS complexes in the posterior leads. This is why half of a millimeter of STE is significant in these leads!
However, these low-voltage leads can make ST-segment elevation difficult to appreciate, which has the potential to confuse the diagnosis. As a result, some experts suggest that the diagnosis of posterior STEMI can and should be made using the other two criteria alone.
Prehospital Thrombolytics
Over the last ten years, the use of thrombolytics in the prehospital arena has increased significantly around the world, especially in rural and remote communities.
While primary-PCI within 120 minutes of first-medical contact (FMC) remains the ideal pathway for patients with acute STEMI, a combined pharmaco-invasive approach has been suggested to be comparably effective in reducing morbidity/mortality in patients presenting with acute STEMI in regions that cannot provide primary-PCI.
In these cases, patients are treated with intravenous fibrinolytics, usually following ECG transmission, expert consultation, and careful screening processes. Following this, the patient is promptly arranged transport to a PCI center where rescue catheterization or follow-up angiogram can be completed.2
With the goal being to minimize infarction size and myocardial necrosis, many services have implemented protocols that allow for EMS administration of fibrinolytics. This has been shown to significantly reduce the time-to-treatment when compared to services which transport to the closest facility prior to the administration of fibrinolytics.3
When paramedics are given the appropriate level of training and equipment, prehospital fibrinolysis can be an effective and efficient means of reducing total ischemic time, and efforts should be made to lobby for this intervention in regions which cannot meet the 2-hour PCI window.
Reperfusion Arrhythmias
Between 80-90% of STEMI patients who receive either PCI or thrombolytics will experience some form of reperfusion-related arrhythmias within the first 48 hours of treatment.
With the expanding utilization of thrombolytics for acute STEMI, the occurrence of these “reperfusion rhythms” has become increasingly common in prehospital and ED settings alike. These rhythms most commonly occur when oxygenated blood begins flowing through previously occluded coronary arteries, and while it’s uncertain what degree of coronary artery patency they represent, it’s generally accepted that these arrhythmias represent some degree of myocardial reperfusion.4
Slower reperfusion arrhythmias such as sinus bradycardia and ventricular escape rhythms are thought to be resultant of increased vagal tone in the recently ischemic myocardial tissue; a phenomenon known as the Bezold-Jarisch Reflex, which is most commonly seen in inferior or posterior MI’s.5
These slow rhythms often occur alongside periods of frank hypotension, however these incidents are most often self-limiting and well tolerated, and may in fact occur at a time when the patient reports finally feeling better! Consequently, aggressive interventions to increase the heart rate are rarely required, and can usually be limited to postural changes or the administration of atropine, or very rarely transcutaneous pacing. 7
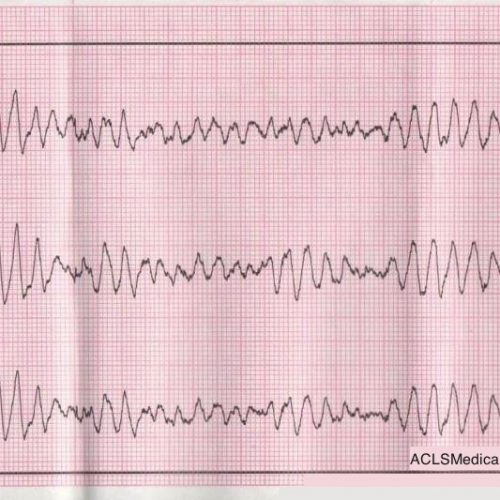
Faster reperfusion arrhythmias may include frequent premature ventricular complexes, accelerated idioventricular rhythm, or nonsustained runs of ventricular tachycardia. These “irritable” rhythms are thought to originate from the zone of ischemia, which surrounds the zone of infarction, where “overactive” calcium channels are believed to play a significant role. The arrhythmia may be occurring as a result of an ectopic foci, or serving as an escape rhythm when the sinus node is depressed (perhaps due to the vagal response mentioned above).
Recent research suggests that the presence of these arrhythmias may predict a larger area of infarction, or possibly incomplete or poor reperfusion (TIMI flow grade <3). Management of these patients should be aimed primarily at continuous cardiac monitoring and hemodynamic support to maximize myocardial perfusion, with use of antiarrhythmic drugs to be considered further down the treatment algorithm.
References
- Oraii S, Maleki M, Abbas Tavakolian A, et al. “Prevalence and outcome of ST-segment elevation in posterior electrocardiographic leads during acute myocardial infarction.” J Electrocardiol 1999;32: 275-8 http://www.ncbi.nlm.nih.gov/pubmed/10465571
- Danchin N, Durand E, Blanchard D, “Pre-hospital thrombolysis in perspective.” European Heart Journal. DOI: http://dx.doi.org/10.1093/eurheartj/ehn462 2835-2842 First published online: 23 October 2008
- McCaul M, Lourens A, Kredo. “Pre-hospital versus in-hospital thrombolysis for ST-elevation myocardial infarction.” Cochrane Database Syst Rev. 2014 Sep 10;9:CD010191. doi: 10.1002/14651858.CD010191.pub2 http://www.ncbi.nlm.nih.gov/pubmed/25208209
- Ersan Tatli, Güray Alicik, Ali Buturak, Mustafa Yilmaztepe, and Meryem Aktoz, “Arrhythmias following Revascularization Procedures in the Course of Acute Myocardial Infarction: Are They Indicators of Reperfusion or Ongoing Ischemia?,” The Scientific World Journal, vol. 2013, Article ID 160380, 7 pages, 2013. doi:10.1155/2013/160380 http://www.hindawi.com/journals/tswj/2013/160380/cta/
- Koren G, Weiss AT, Ben-David Y, Hasin Y, Luria MH, Gotsman MS. “Bradycardia and hypotension following reperfusion with streptokinase (Bezold-Jarisch reflex): a sign of coronary thrombolysis and myocardial salvage.” http://www.hindawi.com/journals/tswj/2013/160380/cta/
- Gulumser Heper, Mehmet Emin Korkmaz, Ayhan Kilic, “Reperfusion Arrhythmias: Are They Only a Marker of Epicardial Reperfusion or Continuing Myocardial Ischemia After Acute Myocardial Infarction?” ANGIOLOGY 2008 vol. 58 no. 6 663-670 doi: 10.1177/0003319707308891 http://ang.sagepub.com/content/58/6/663
- Esente P, Giambartolomei A, Gensini GG, Dator C. “Coronary reperfusion and Bezold-Jarisch reflex (bradycardia and hypotension)”, Am J Cardiol. 1983 Aug;52(3):221-4. http://www.ncbi.nlm.nih.gov/pubmed/6869265

Comments