Unfortunately not every patient that suffers a STEMI makes a complete recovery, even if treated with primary PCI. Patients that present late into their infarct have a higher risk of developing a complication.
Here are two cases that illustrate the spectrum of mechanical complications that can occur in the aftermath of an infarct.
Case 1
A 53 year old lady with hypertension and hypercholesterolaemia called an ambulance about 8 hours after the onset of her chest pain.
Vital signs are assessed.
BP: 100/60
HR: 96bpm
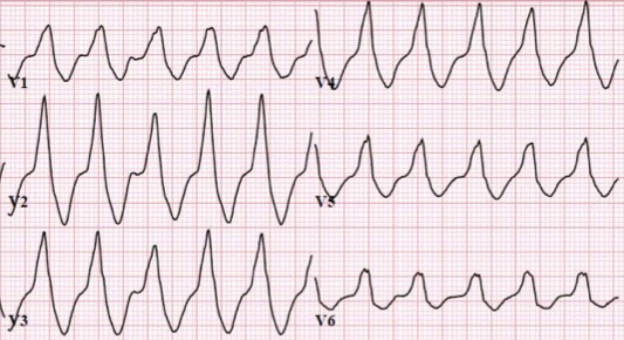
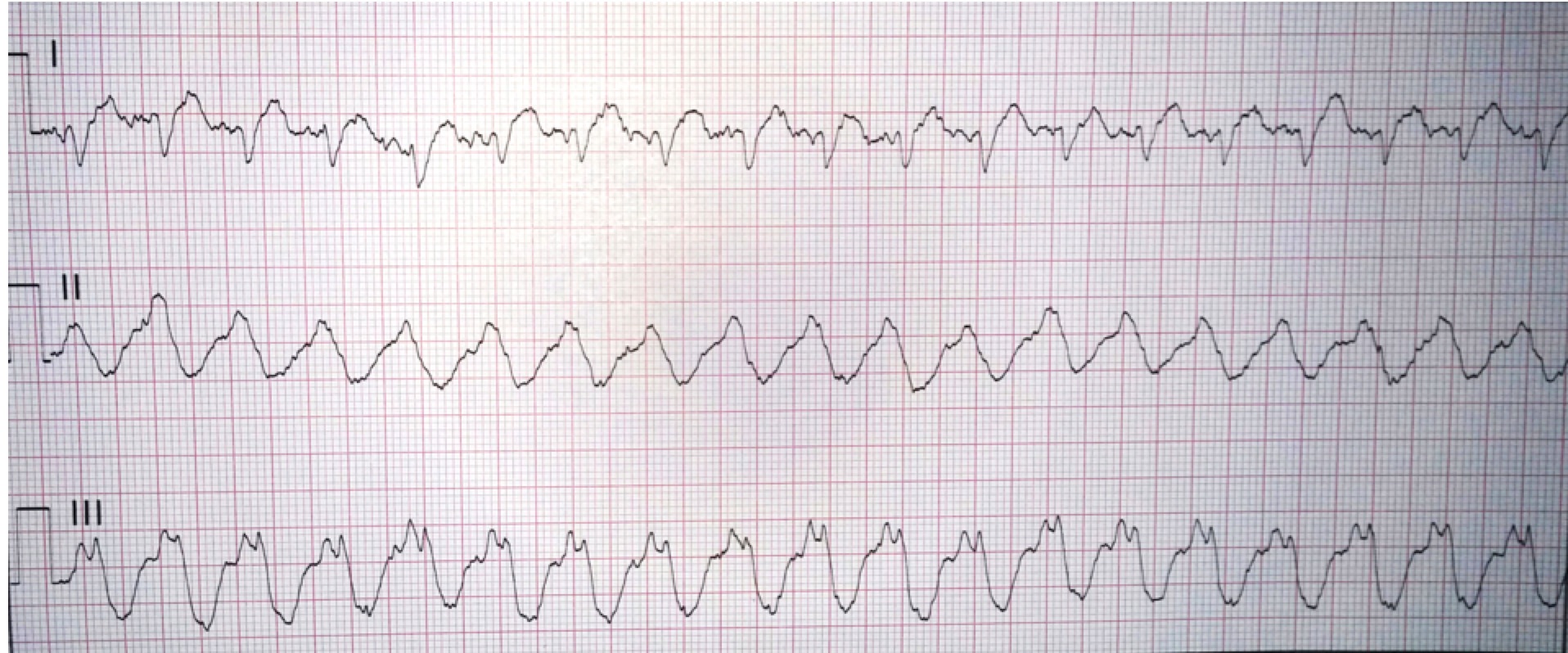
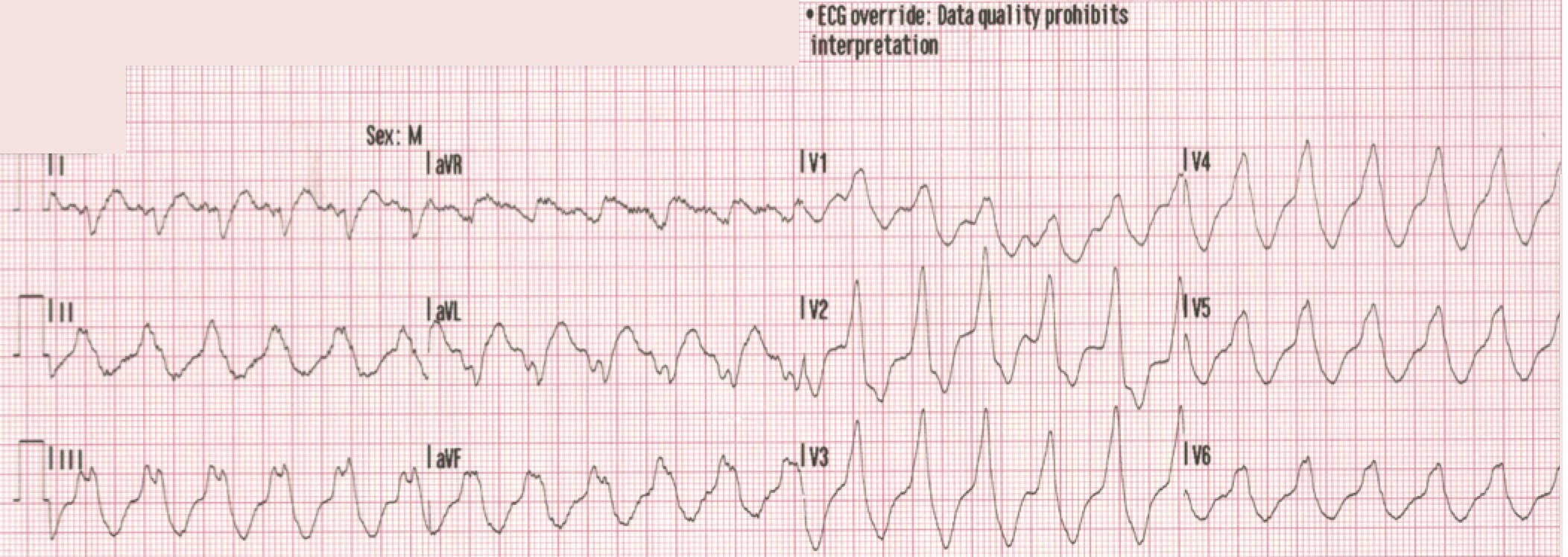
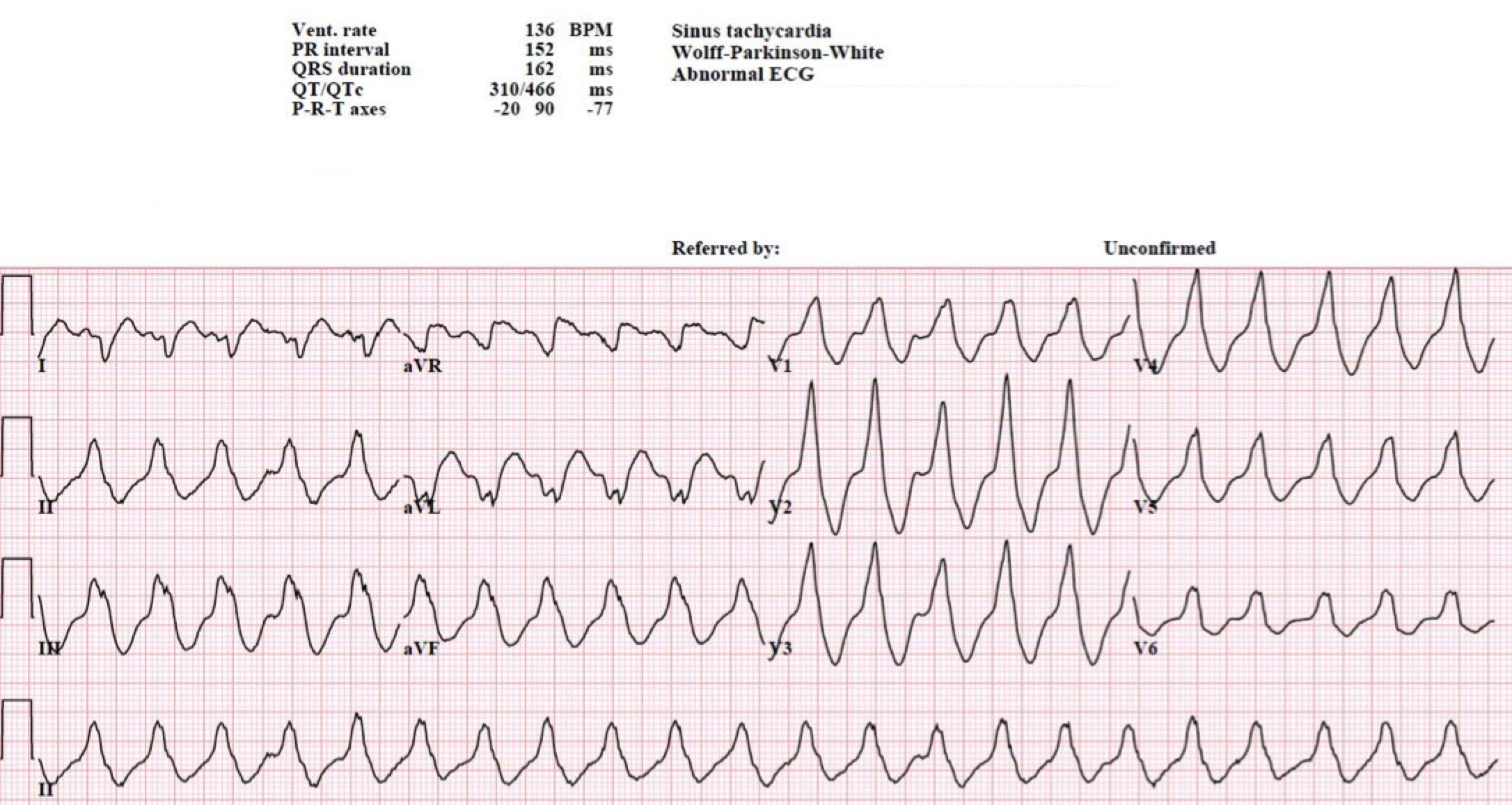
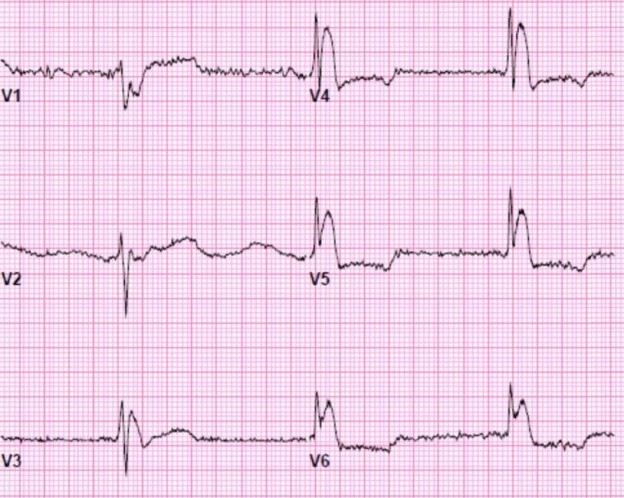
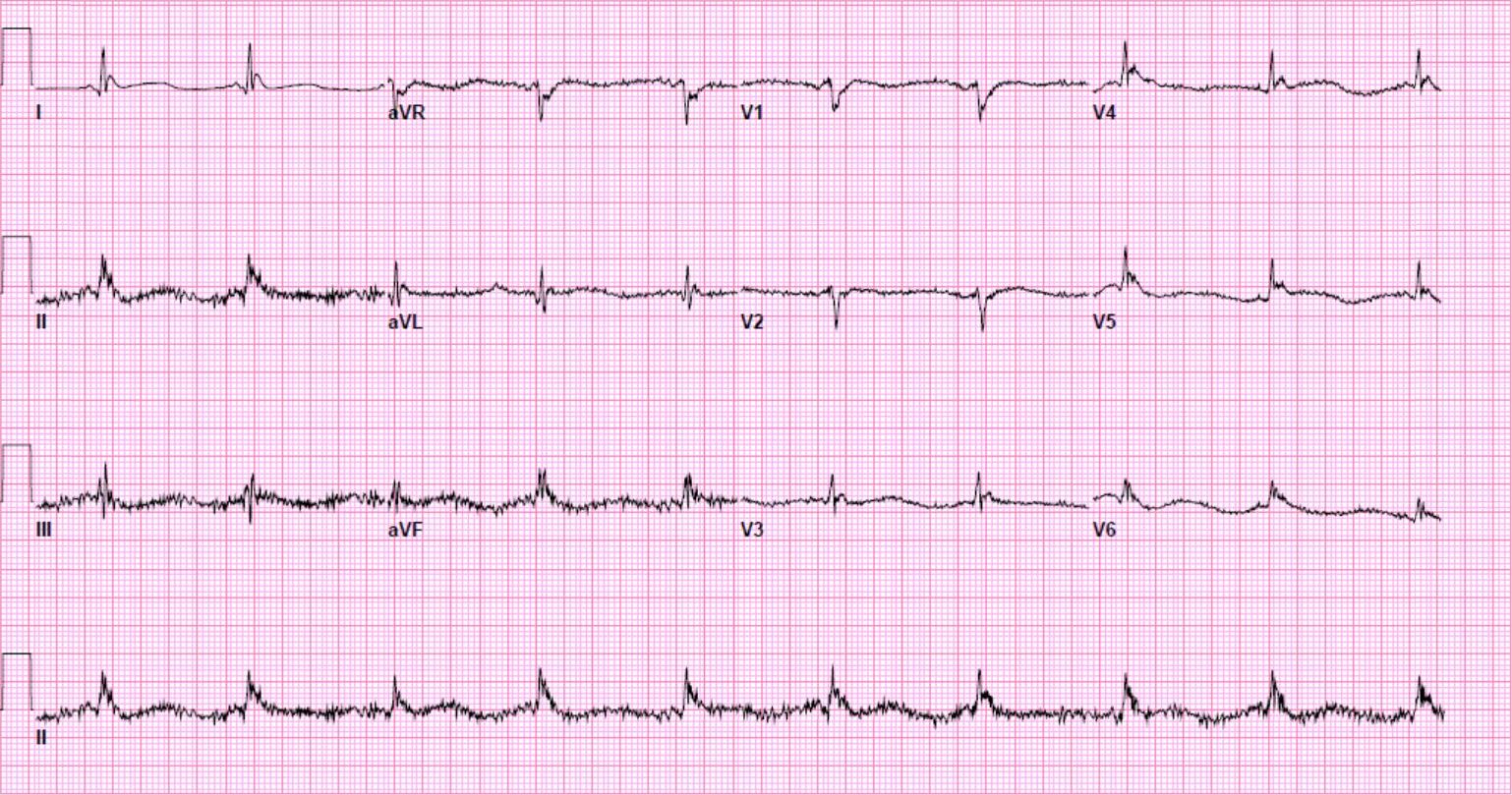
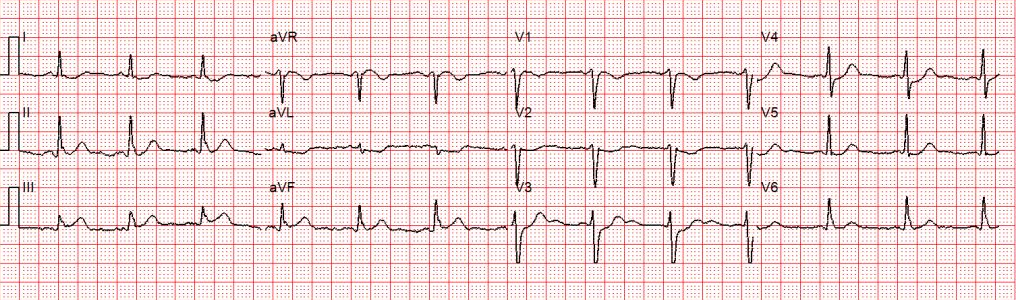
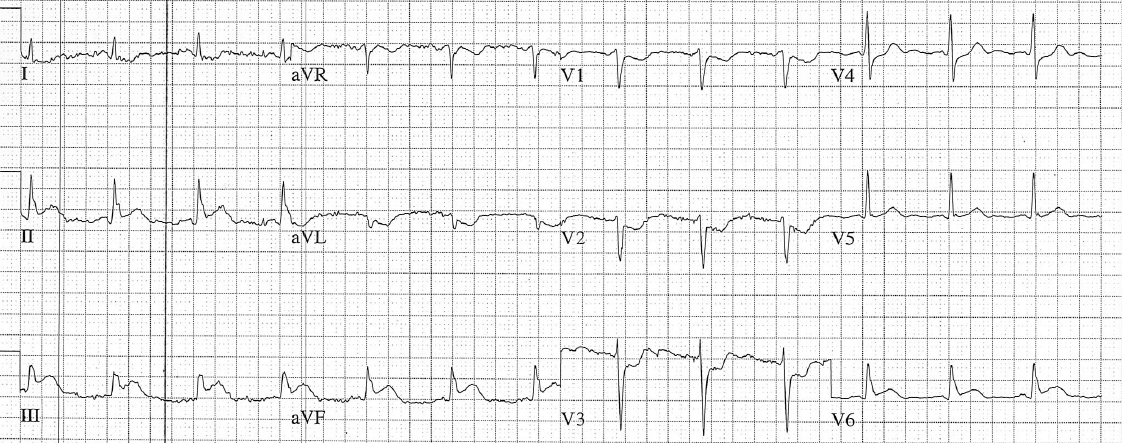
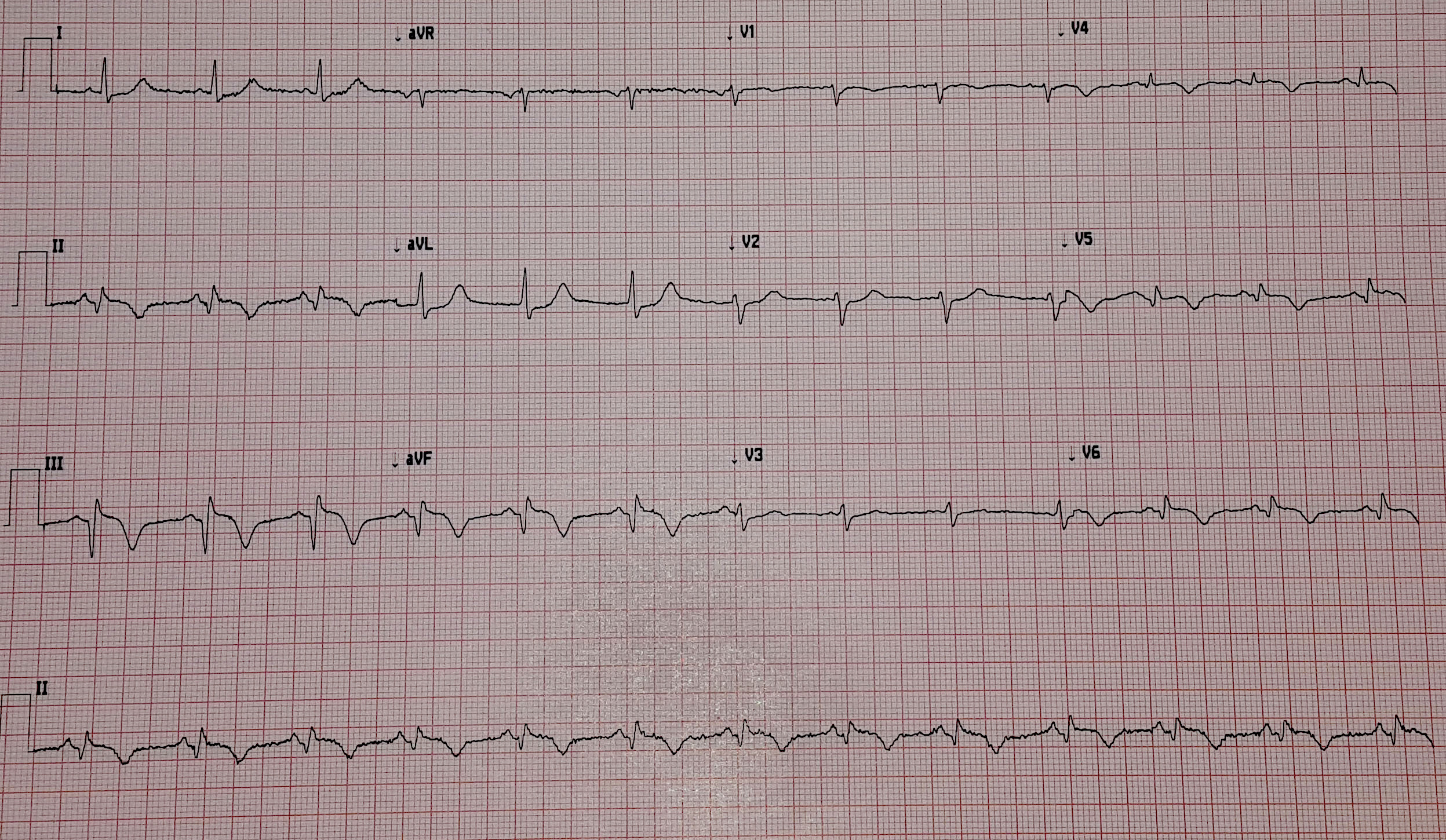
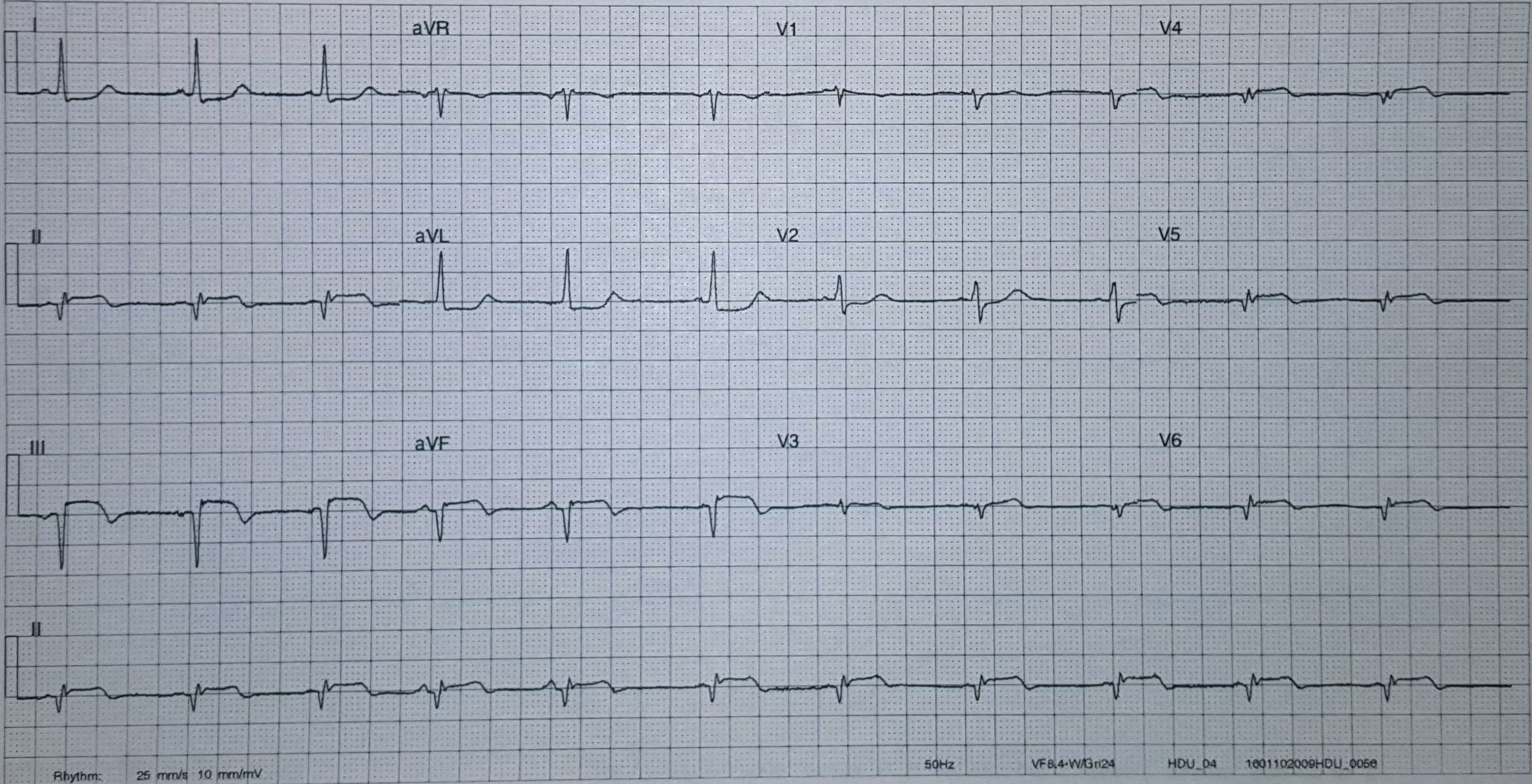
The pre-hospital ECG traces obtained by the paramedics are shown:
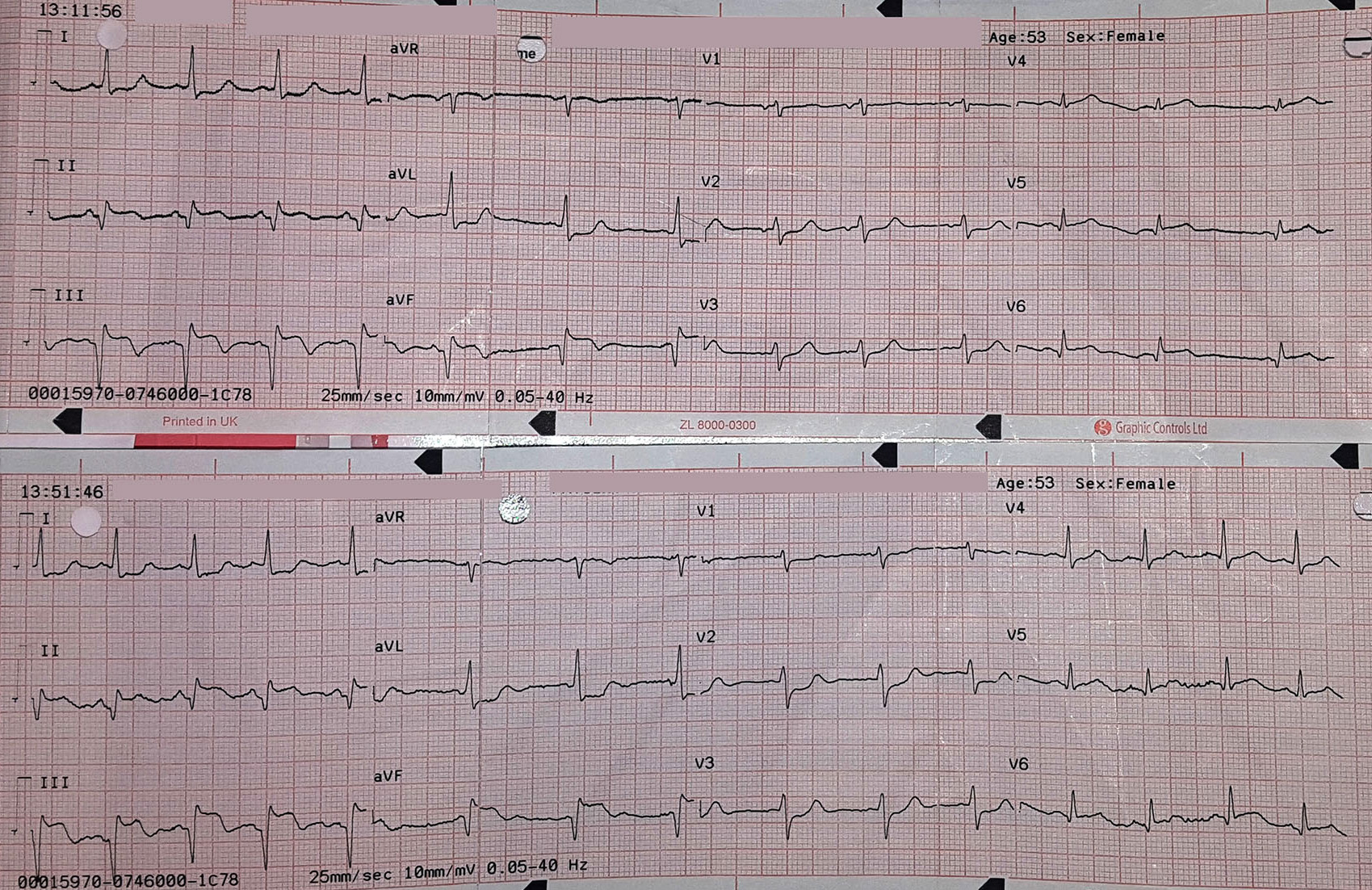
Both ECGs show clear inferior ST elevation with prominent Q waves. There is reciprocal change anterolaterally but importantly for an inferior MI, heart rate is normal. The ECGs are 50 minutes apart and the changes appear to be slightly worse on her second ECG, but not drastically.
She was still in pain on arrival at the interventional centre and transferred immediately to the cath lab. Her left system showed moderate disease in the circumflex artery. However, as expected, the acute problem was her right coronary artery, which was occluded.
Below you can see the guide catheter engaged with the blocked right coronary artery and no flow is getting past the clot.
A thin angioplasty wire is passed through the thrombus and to the distal vessel. The thrombus was more resistant (i.e. mature) than most acute infarcts, which fit with the 8 hour history of pain.
You can see even passing a 0.014” diameter wire restores some flow. The wire tip is in the posterior descending artery. Reperfusion is often when patients destabilise and indeed the patient’s heart rate dropped to 20bpm and blood pressure to 60mmHg but she responded quickly to atropine and fluid. In the proximal vessel, a filling defect can be seen which is a sizeable thrombus.
A 3.5mm wide and 38mm long drug-eluting stent was placed without complication in her RCA, producing a nice angiographic result. However, the long period of coronary occlusion may well have caused significant myocardial injury. She was kept under close observation.
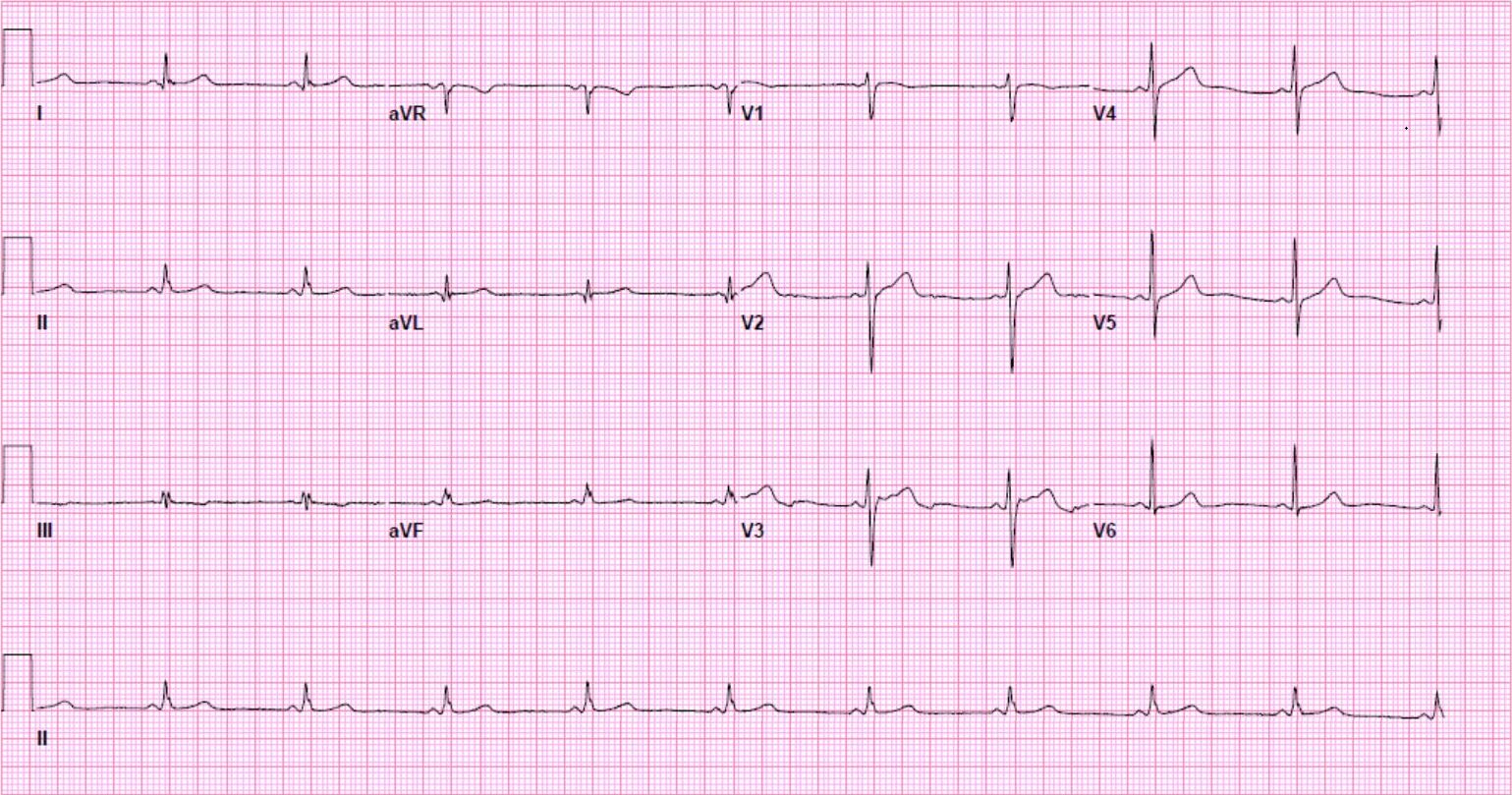
A satisfying sight for any healthcare professional is seeing a patient’s ST elevation resolve after opening their artery. However, her post procedure ECGs revealed persistent ST elevation.
You can see the evolution of her infarct as the deeply inverted inferolateral T waves revert but her STs remain elevated and develop a more mature ‘rounded’ appearance.
She returned to the ward but deteriorated. Inferior STEMIs carry a more favourable prognosis than anterior (as LV function is normally not as dramatically affected), so clinical instability post procedure should be a concern. On examination she was pain-free but breathless:
RR 24
SO2 92% 2L O2
HR: 80bpm
Chest auscultation: crackles bibasally
Heart sounds: loud pansystolic murmur
A bedside echocardiogram was performed.
A parasternal long axis view reveals the posterior mitral valve leaflet is tethered. The basal posterolateral wall is hypokinetic.
A close up of the valve with colour Doppler demonstrates mitral regurgitation.
An apical 4-chamber (zoomed in) shows the mitral regurgitation is significant.
This parasternal short axis view gives the clearest demonstration of the problem. A regional wall motion abnormality is clearly seen affected the infero-septum and inferior wall. The rest of the left ventricle is contracting well.
Her chest radiograph confirmed the clinical suspicion of pulmonary oedema and she was treated with diuresis. She responded well.
Why did the patient develop pulmonary oedema?
The papillary muscles are very strong muscles connected to the mitral valve to prevent it inverting during ventricular systole. There are two papillary muscles in the left ventricle, each connected to a mitral valve leaflet.
The anterolateral papillary muscle is connected to the anterior mitral valve leaflet and receives a blood supply from both the left anterior descending artery (via a diagonal) and the circumflex artery (via an obtuse marginal). However the posteromedial papillary muscle only has one blood supply, which is the posterior descending artery, a branch of the right coronary artery in 90% of people.
Therefore one can appreciate why mitral valve problems are more common following an inferior STEMI. In this case an almost akinetic segment, which included the posteromedial papillary muscle, caused the posterior mitral valve leaflet to become fixed, causing mitral regurgitation. Even though overall left ventricular function was only mildly impaired on the echocardiogram, the regurgitant pressure into the lungs can precipitate pulmonary oedema.
In more severe cases, the papillary muscle may rupture completely causing a ‘flail leaflet’ and catastrophic mitral regurgitation. It is often fatal. This complication typically occurs 2-7 days following a myocardial infarction, so if a patient suddenly deteriorates in the days after an MI, check for a murmur and organise an urgent echocardiogram. They can develop cardiogenic shock within minutes.
Case 2
An 80 year old man suffered a severe episode of chest pain but did not seek medical attention until about 2 weeks later, by which time he’d become progressively more breathless. His primary care doctor heard a loud, previously undocumented murmur and referred him into hospital.
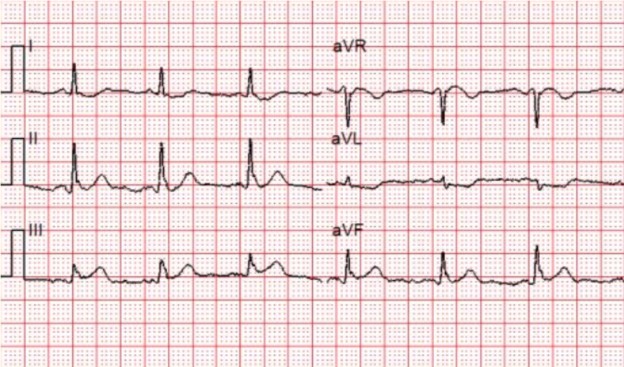
On examination, in addition to the murmur, he had signs of right sided heart failure with an elevated JVP and peripheral oedema. His ECG revealed inferior Q waves.
Parasternal long axis view: The septum is moving in an unusual jerky fashion and something can be seen in the RV. Despite left ventricular function appearing reasonable, the aortic valve is not opening much suggesting cardiac output is low.
Parasternal short axis: There is a large ventriculo-septal defect in the infero-septal LV. The right ventricle is severely impaired.
Apical 4 chamber:
The LV function is hyperdynamic. The infero-basal septum is tethered near the mitral and tricuspid valves but highly mobile, creating a large VSD. The right ventricular free wall appears to bulge out and the RV is almost akinetic.
Apical 4 chamber colour Doppler:
There is free flow between LV and RV.
Apical 2 chamber. This view demonstrates the bulging from the RV also appears to involve the LV. This is a sealed perforation with aneurysm formation.
In this remarkable loop, the echo probe moves and one can clearly appreciate the defect in the septum, along with the thin membranes sealing the perforation.
What happened?
In addition to problems with the mitral valve, ventricular perforation and ventriculoseptal defects (VSDs) are the two other catastrophic mechanical complications of an MI. LV wall rupture typically occurs in the first 5 days, but some can be as late as a fortnight later. In this case, it is unclear when the complication occurred.
Complete free wall rupture rapidly leads to tamponade and death, but a sub-acute perforation refers to one that has been sealed with thrombus or the pericardium. This remains very high risk for subsequent complete rupture. Somewhat paradoxically the risk of developing any mechanical complication is not proportional to the size of the infarct and small infarcts can pose a large risk.
This patient suffered both a large VSD and a sealed perforation of the inferobasal free wall.
Management
These patients may present in cardiogenic shock and should be managed accordingly. Treatment might include diuresis, vasopressors, inotropes, intra-aortic balloon pump or mechanical cardiac support. The only definitive treatment is invasive, but these patients are exceedingly high risk and optimal timing can be very hard to judge. Most patients will be considered for early surgery but percutaneous closure of VSDs is increasing, to avoid the risk of a general anaesthetic.
Summary
- There are three mechanical complications of acute myocardial infarction: acute mitral regurgitation, VSD and LV rupture
- They typically occur 2-7 days following an MI
- Have a high index of suspicion if a patient presents following an MI with a sudden deterioration
- Symptoms and signs include breathlessness, right-sided heart failure and a new harsh pansystolic murmur
- Urgent echocardiography is indicated and diagnostic in most cases
- Treatment is supportive and surgical
References:
Mechanical complications of acute myocardial infarction, accessed 26th February 2016. Available at: http://www.uptodate.com/contents/mechanical-complications-of-acute-myocardial-infarction